- All prosthetic heart valves have an expected amount of stenosis.
- Prosthetic valves are designed to have a small amount of regurgitation, i.e. “physiological closing volume.”
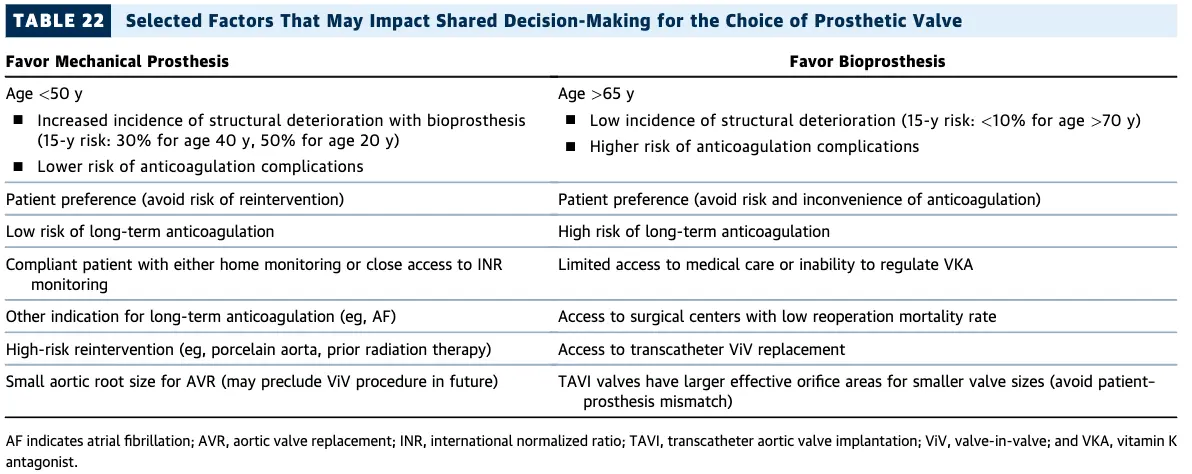
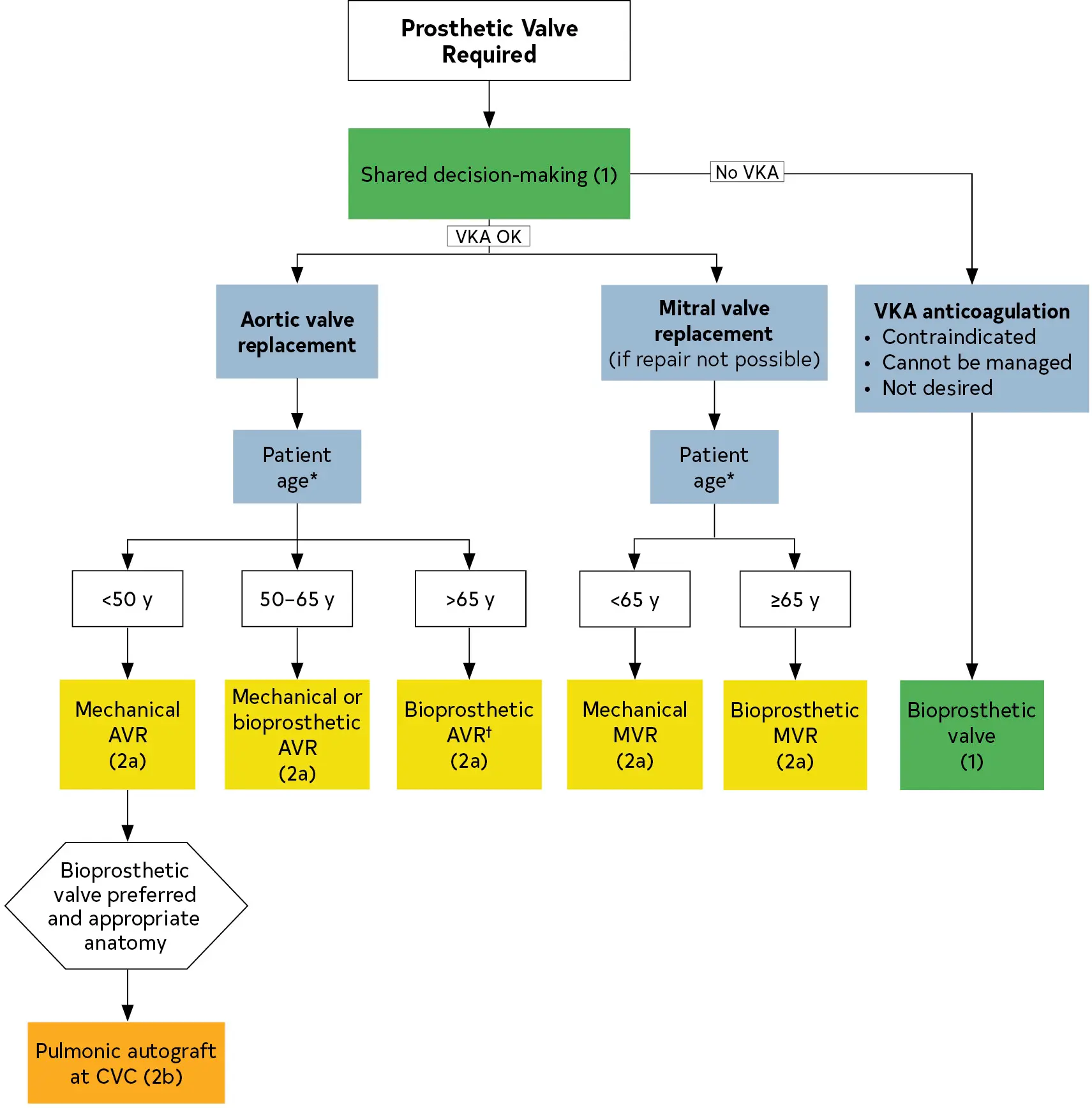
Which valve should they get?
Management
- Asymptomatic patients can generally be followed with a clinician examination annually.
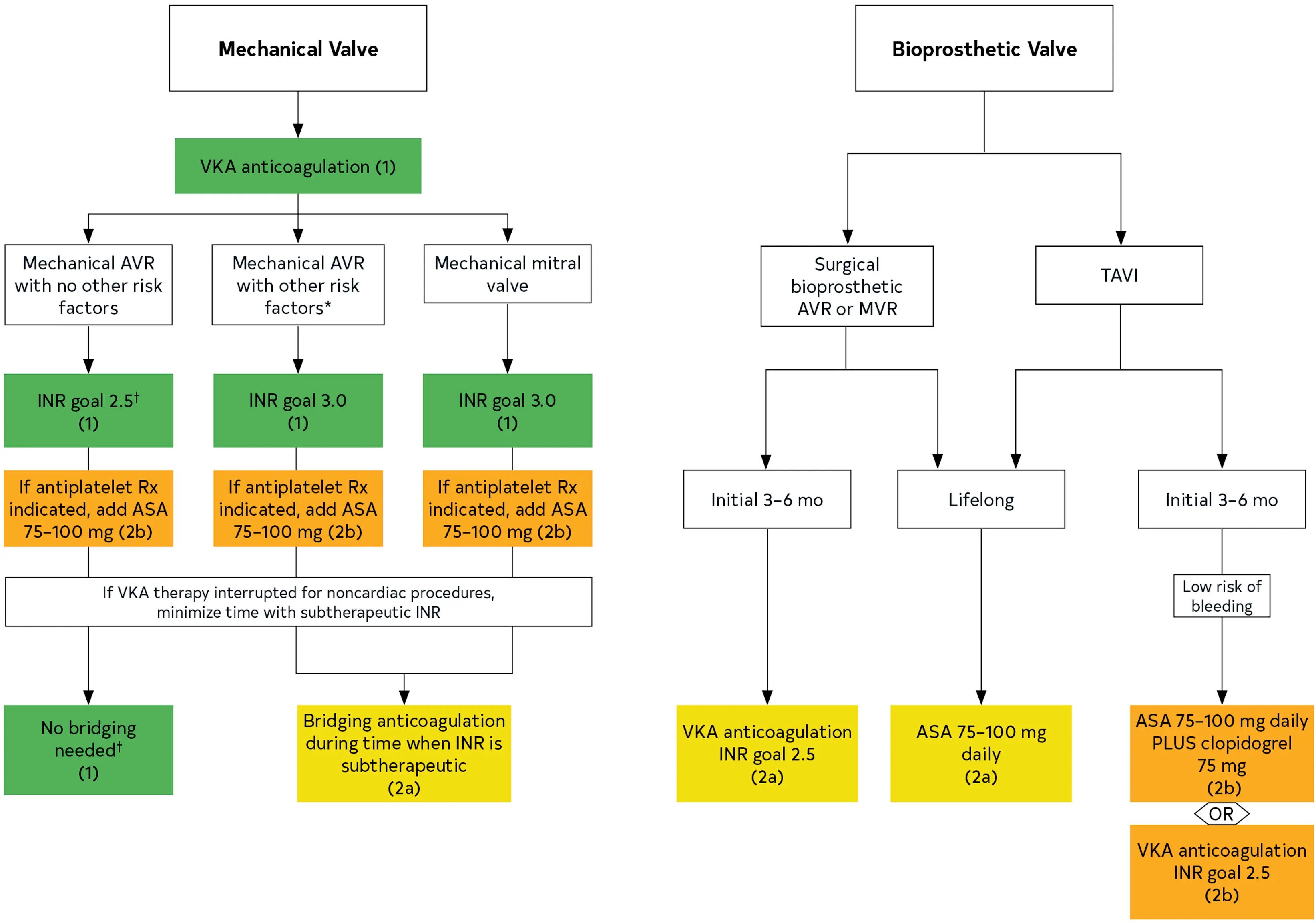
Anticoagulation
- In patients with a mechanical prosthetic valve, anticoagulation with warfarin is recommended (Class 1)
- Bioprosthetic valves
- TAVI:
- if low risk of bleeding, DAPT with aspirin 75 to 100 mg daily + clopidogrel 75 mg daily for 3-6 months post-implantation (Class 2a)
- aspirin 75 to 100 mg daily is reasonable (Class 2a)
- Bioprosthetic SAVR:
- TAVI:
Endocarditis Prophylaxis
Echo Surveillance
- Initial Echo
- “In patients with a surgical or transcatheter prosthetic valve and in patients who have had valve repair, an initial postprocedural TTE study is recommended for evaluation of valve hemodynamics and ventricular function” (Class 1)
- Surveillance Echo
- Guidelines recommend a follow-up echocardiogram 4-12 weeks after valve surgery to establish a new baseline.
- Waiting several weeks allows for recovery of anemia, stabilization from any early postoperative fluid shifts, and stabilization from perioperative medications, which may alter valvular gradients and/or ventricular mechanics early on.
- Bioprosthetic valves
- In patients with a bioprosthetic surgical valve, TTE at 5 and 10 years and then annually after implantation is reasonable, even in the absence of a change in clinical status. (Class 2a)
- In patients with a bioprosthetic TAVI, TTE annually is reasonable (Class 2a)
- Guidelines recommend a follow-up echocardiogram 4-12 weeks after valve surgery to establish a new baseline.
- Clinical deterioration → get a TTE (Class 1)
- If TTE doesn’t show valve dysfunction, get additional imaging (TEE, gated cardiac CT, or fluoro) (Class 1)
Bioprosthetic Valves
-
Surveillance Echo