# Endocarditis
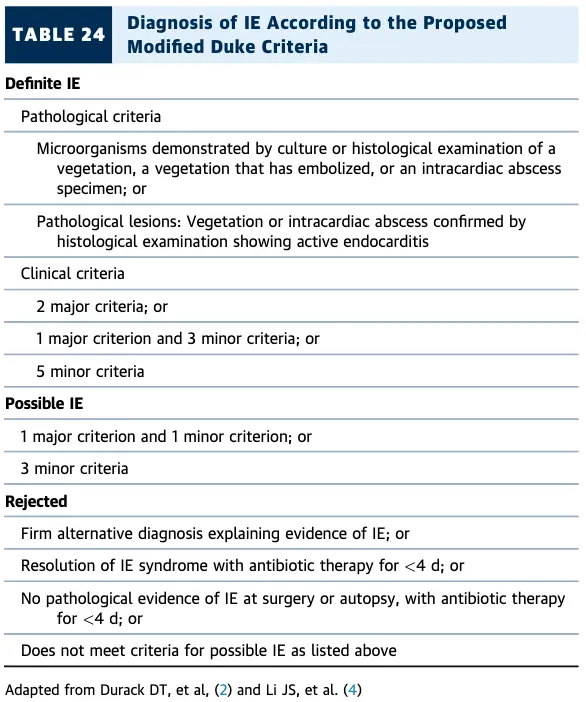
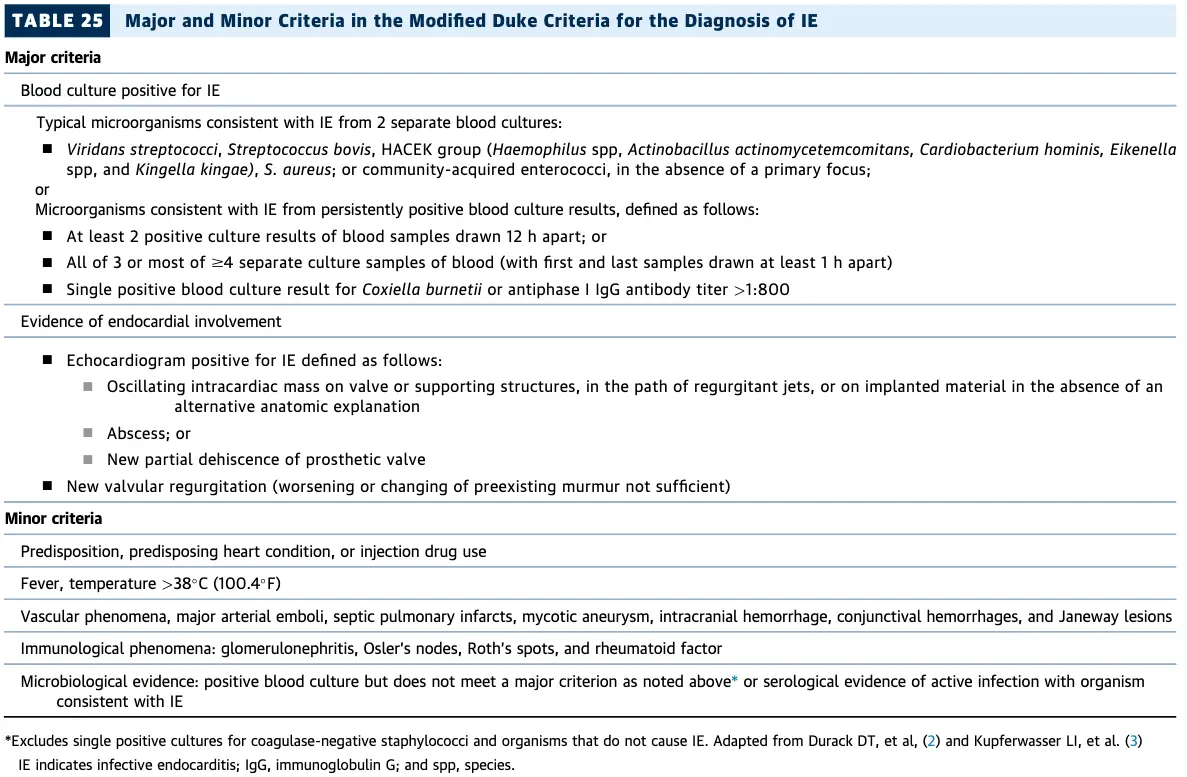
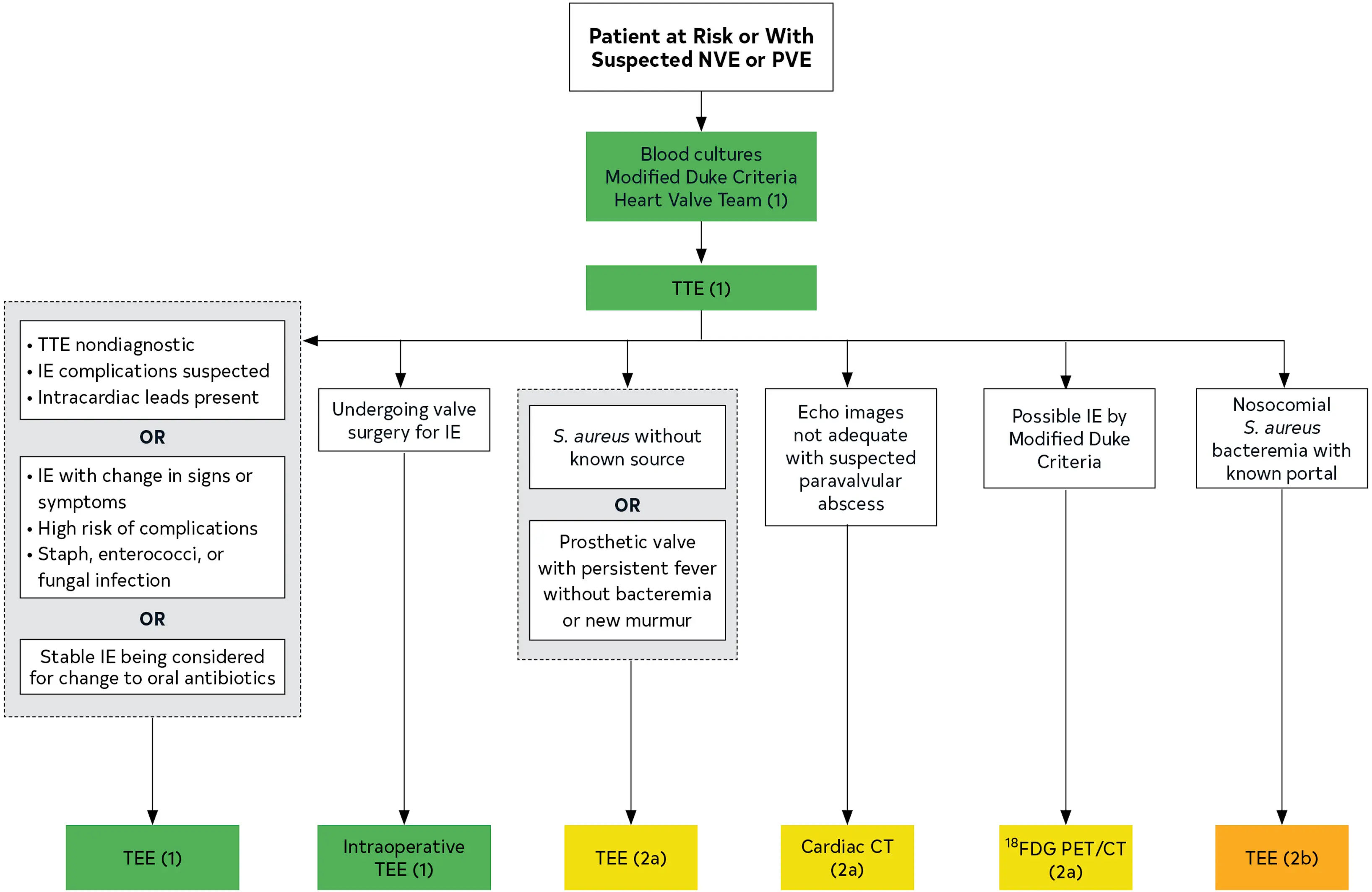
- Modified Duke Criteria: ***
- If possible IE, plan for FGD-PET/CT
- BC x2
- TTE ordered to assess for vegetations, characterize the hemodynamic severity of valvular lesions, assess ventricular function and pulmonary pressures, and detect complications
- If TTE nondiagnostic, plan to proceed with TEE
- If paravalvular infection suspected, will order CT- TEE has better sensitivity for detecting bacterial endocarditis compared to TTE
- Native valve vs. Prosthetic valve? - Timing of infection after valve intervention?
- Fatal if untreated
- in-hospital mortality rate is 15% to 20%, with a 1-year mortality rate approaching 40% 1
Diagnosis
Modified Duke Criteria
Management
Complications
- Progression to involve the valve annulus → fistula between the LA and LV, which could result in significant regurgitation.
Footnotes
-
Otto, C. M., Nishimura, R. A., Bonow, R. O., Carabello, B. A., Erwin, J. P., Gentile, F., Jneid, H., Krieger, E. V., Mack, M., McLeod, C., O’Gara, P. T., Rigolin, V. H., Sundt, T. M., Thompson, A., & Toly, C. (2021). 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease. Journal of the American College of Cardiology, 77(4), e25–e197. https://doi.org/10.1016/j.jacc.2020.11.018 ↩