Acute MR
- Common causes include:
- Endocarditis
- Papillary muscle rupture or chordal muscle rupture, e.g. after recent MI or infarction
- Can result in flail leaflet
- Sudden ↑ in LA and LV volume in the absence of compensatory LV or atrial dilation.
- Management
- Urgent surgery
Post-MI Mitral Regurgitation
Papillary muscle rupture
- Complicates 1-5% of acute Medications
- Usually 2-7 days after the acute ischemic event; typically first MI
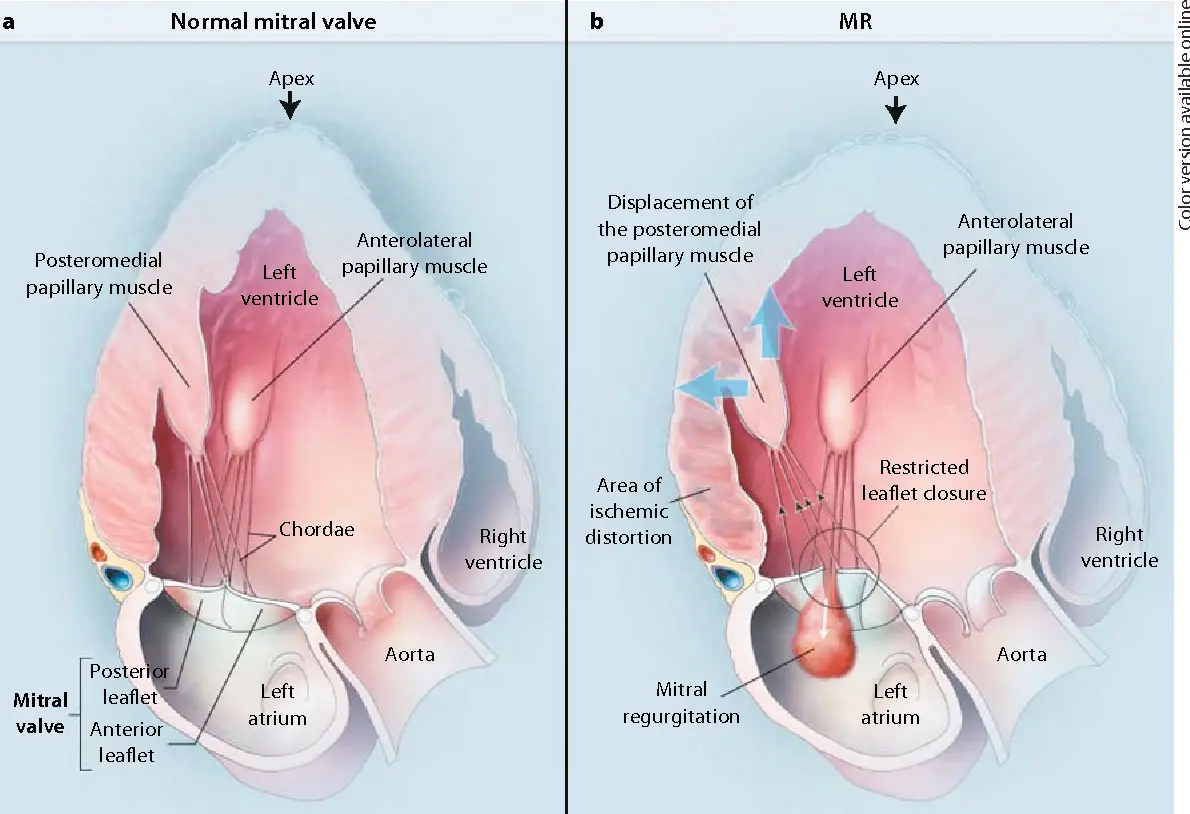
- Posteromedial papillary muscle more commonly ruptured (10x more likely) due to have single blood supply (posterior descending artery)
- The anterolateral papillary muscle has dual blood supply
- ⚠️ Exam may not have feature a hyperdynamic precordium or audible murmur
- d/t rapid and complete equalization of pressure between the LV and LA.
- By contrast, ventricular septal rupture would present similarly, but you’ll hear a loud murmur.
Ischemic Mitral Regurgitation
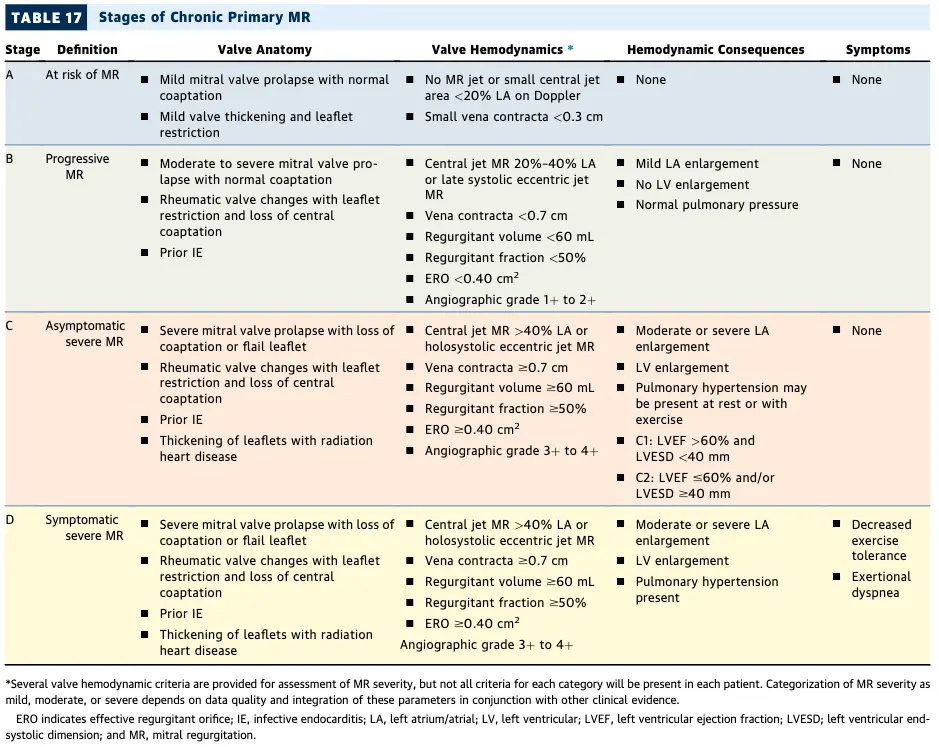
Chronic Mitral Regurgitation
- “If you see MR, you need to ask why?”
- “A comprehensive evaluation of valvular regurgitation should include identifying the mechanism and the severity of valvular regurgitation, along with adaptation of the heart to the volume overload.”
- Results in LV volume overload → ventricular (and atrial) remodeling w/ eccentric hypertrophy, i.e. LV dilation w/o increased wall thickness.
- Can be tolerated for several years. Only after several years (typically), may it lead to ↓ contractility and systolic dysfunction → ↑ pulmonary venous pressure, ↓ SV and ↓ CO.
- ↑ LAP: pulmonary congestion, pulmonary hypertension, and atrial fibrillation
4, 5, 6, 7 of Severe MR
EROA ≥ 0.4 cm2 Regurgitant fraction ≥ 50% Regurgitant volume ≥ 60 mL Vena contracta ≥ 0.7 cm
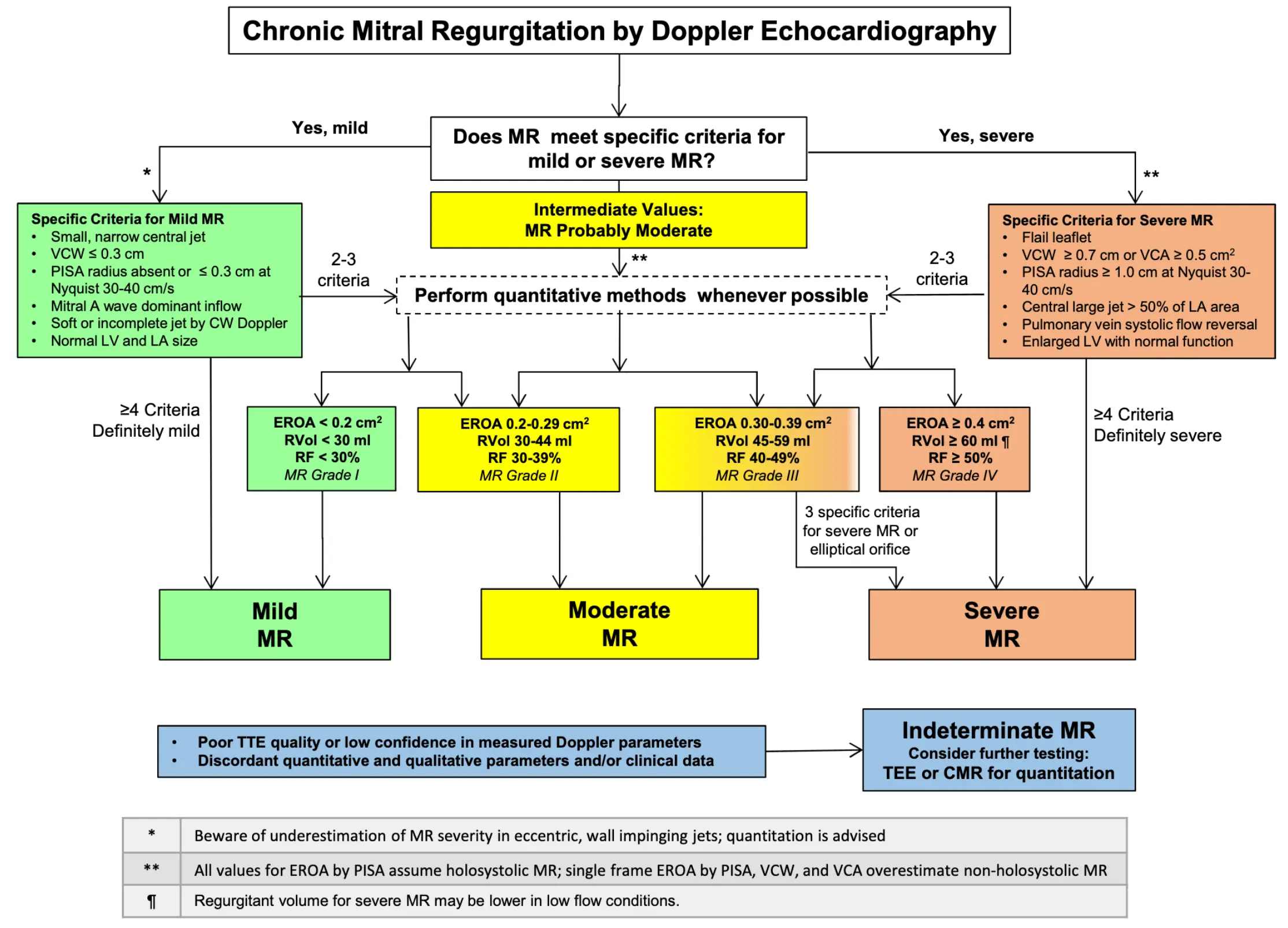 Source: Figure 18 of 2017 ASE Valvular Guidelines
Source: Figure 18 of 2017 ASE Valvular Guidelines
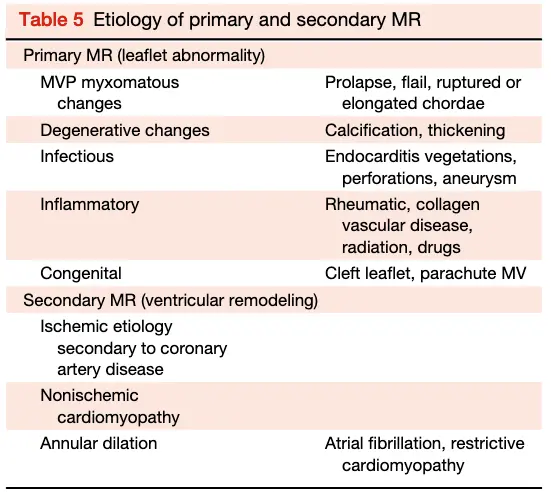
- Primary or Secondary (functional) MR?
- differentiates 1˚ lesions of the mitral leaflets and subvalvular apparatus from 2˚ dysfunction d/t annular or LV dilatation/remodeling and/or dysfunction.
- Most common causes of MR: Secondary MR is the most prevalent form of MR, followed by Mitral Valve Prolapse (MVP), ischemic MR.
- Primary MR includes:
- myxomatous ∆, notably Mitral Valve Prolapse (MVP)
- Mitral Annular Calcification (MAC)
- Rheumatic Heart Disease
- Connective Tissue Disease
- radiation therapy ☢️
- adverse effects of medications 💊
- Echo
- Don’t forget to provide information regarding the associated conditions or sequelae of MR, such as pulmonary hypertension, tricuspid regurgitation, LA dilation, and ventricular dilation or systolic dysfunction
- ⚠️ In the presence of severe primary or secondary MR, use of LVEF may overestimate systolic function because of the lower impedance of the LA chamber.
- Be sure to check LVESD
- TEE can also be helpful given its ↑ spatial resolution and the proximity of the probe to the MV.
- MV surgical views are 🔥
- Echo Doppler
- vena contracta width, ERO, spatial distribution of MR jet w/in the LA, flow convergence
- Screening
- After the initial echocardiographic evaluation, repeat echocardiography is indicated for patients with moderate or greater MR, even in the absence of symptoms
- Frequency
- Severe MR: every 6-12 months
- Moderate MR: every 1-2 years
- Mild MR: every 3-5 years
- ⚠️ Repeat echocardiography is also recommended for patients with any degree of MR and a change in clinical status or physical examination findings.
Primary Mitral Regurgitation
“Primary MR is a fancy way for saying prolapse.”
- David Skolnick, August 9, 2024
| Etiology | Affected Valve Level(s) |
|---|---|
| Degenerative (see MVP) | leaflets, chordae, annulus |
| Mitral Annular Calcification (MAC) | annulus, leaflets |
| CAD → ruptured papillary mm. | papillary mm. |
| Rheumatic Heart Disease | leaflets, chordae |
| Endocarditis | leaflets, chordae |
| Hypertrophic Cardiomyopathy | leaflets, chordae, papillary mm. |
| Connective Tissue Dz (RA, SLE, APLS) | leaflets, annulus |
| Radiation ☢️ | leaflets, chordae |
| Drugs (ergotamines, methysergide, pergolide, fenfen, dexfen) | leaflets, chordae |
- “A mechanical problem requires a mechanical solution”
- Primary MR is a mechanical problem of the leaflet coaptation that only has a mechanical solution, i.e. MV intervention
- Primary MR is a mechanical problem of the leaflet coaptation that only has a mechanical solution, i.e. MV intervention
Secondary Mitral Regurgitation
- Secondary MR occurs in approximately 65% of cases reported with left ventricular dysfunction or remodeling as the predominant cause.
